AI-Driven Virtual Health Systems Integrating Federated Learning for Decentralized Telemedicine
Authors :
Sulaiman Bruggen and Venkata Sah
Address :
College of Technological Innovation, Zayed University, UAE
Department of Computer Science and Engineering, Indian Institute of Technology (Indian School of Mines), Dhanbad, Jharkhand, 826004, India
Abstract :
Telemedicine is using telecommunications and digital technologies to deliver healthcare services remotely. Integrating Artificial Intelligence (AI) in telemedicine has revolutionized virtual health systems by enabling personalized and efficient healthcare delivery. However, centralising medical data raises significant challenges, including privacy concerns, security risks, and regulatory constraints. Federated Learning (FL) provides a decentralized framework to overcome these challenges by providing collaborative model training across distributed datasets without compromising patient confidentiality. The paper proposes a method, FL-AIVHS, to design an AIdriven virtual health system (VHS) integrating Federated Learning to enhance data security, improve predictive accuracy, and enable equitable access to telemedicine solutions. The FL-AIVHS leverages FL for distributed model training on anonymised patient data from multiple healthcare providers. Advanced deep-learning models like convolutional neural networks (CNN) are utilized for disease prediction, while privacy-preserving techniques are used to ensure data security. Key findings demonstrate a 35% improvement in model accuracy compared to traditional centralized training methods and a significant reduction in privacy breach risks. The system also performs well across different datasets and complies with data protection standards like General Data Protection Regulation (GDPR). In conclusion, the AI-driven virtual health system integrating Federated Learning provides a transformative approach to decentralized telemedicine, addressing privacy, scalability, and accessibility challenges in modern healthcare.
Keywords :
Federated Learning (FL), Virtual Health Systems (VHS), Privacy-Preserving Techniques, Disease Prediction, Decentralized Healthcare, Data Security.
1.Introduction
As a result of the IoMT revolution, which has increased the quality of healthcare services, there have been extensive changes in the way healthcare institutions operate. The use of Internet of Medical Things (IoMT) devices to track and relay a patient's vital signs is on the rise in healthcare [1]. Telemedicine is more helpful than other technologies, as it facilitates preventative care and enhances people's health in the long run. This is particularly true for those learning about regional or financial incentives to obtain high-quality treatment [2]. Overcoming these obstacles and enhancing healthcare delivery in these neglected places is greatly encouraged by the merging of telemedicine and AI. Telemedicine allows for remote consultations and diagnostic services to bridge the gap between healthcare providers and patients in rural areas [3]. Similarly, AI-driven virtual health systems use advanced computational algorithms to analyze patient data, predict outcomes, and support health professionals in making informed decisions. Given the centralized nature of data storage and processing, these are significant challenges with traditional AI. It results in issues regarding data protection, security-related issues, and regulatory concerns [4]. Telemedicine became an important constituent within any modern healthcare system because it could link patients with healthcare providers and minimize constraints linked to the physical place of residence. Some benefits of AI-powered virtual health systems include real-time monitoring, predictive analytics, and automated diagnostics [5].
FL has become a novel solution to these challenges. In contrary to the traditional approach, FL decentralizes the whole training process—that is, individual healthcare service providers working together train AI models keeping private all patient information [6]. This way, it could preserve privacy and ensure full compliance with the regulatory frameworks while allowing diverse datasets for model training. FL can change the face of telemedicine and some of the most pressing limitations in integrating AI-driven virtual health systems [7]. Additionally, users have significant privacy leakage issues since health-related data is collected in their homes and then sent to the health organization for examination [8]. Traditional centralized AI models, while effective, are ill-suited in applications where data sensitivity becomes an issue. The lack of privacy-preserving mechanisms in such systems exposes them to data breaches, bringing down public trust in telemedicine solutions [9].
The FL-AIVHS addresses the challenges of telemedicine in dealing with privacy, security, and scalability issues by integrating Federated Learning into AI-driven virtual health systems. FL enables the training of decentralized AI models using local, anonymized patient data from different healthcare providers, taking away the risks of centralizing sensitive data. FL-AIVHS uses high-end deep learning algorithms to achieve accurate disease diagnosis or predictions, even from diverse datasets, without exposing the raw data. The provided privacypreserving techniques will guarantee the training processes with differential privacy and model updates with homomorphic encryption to ensure the confidentiality of patients. It also strictly complies with regulatory standards, such as GDPR, to ensure compliance while using edge computing for scalability and real-time performance in telemedicine applications. FL-AIVHS, by considering these elements, provides a strong, secure, and efficient framework for decentralized telemedicine that gives everybody equal access to personalized health services, addressing some of the critical challenges in data privacy, predictive accuracy, and system scalability
The significance of the paper is that
The outline of the paper is this: Section I outlines the study's scope and objectives. Section II reviews prior research on AI in telemedicine and Federated Learning. Section III details the FL-AIVHS system. Section IV presents experimental findings. Finally, Section V highlights key contributions and future directions.
2. Related Works
Kadir Muhammad Abdul [10] proposed the widespread adoption of telemedicine in developing countries to maintain basic medical treatment during the COVID-19 outbreak. Patients could get medical advice without having to physically visit a doctor thanks to this method, which used information and communication technologies to enable virtual consultations. The result was an improvement in healthcare access and mental health issues through remote psychiatric consultations. Another big limitation was the general unawareness and lack of knowledge of telemedicine among people, which restrained its effectiveness in implementing and using it to handle the challenges thrown up in health care by the pandemic.
Ezeamii, Victor C., et al. [11] proposed the adoption of telemedicine to improve healthcare delivery and patient outcomes. This was explored through a systematic review of empirical studies that utilized quantitative and qualitative methods to assess the impact of telemedicine on various patient populations. The results showed significant improvements in patient engagement, satisfaction, and management of chronic diseases, especially in diabetes care. The study was, however, constrained by limitations of the included research, variability in telemedicine practices, and challenges to ensure equitable access, which have been underlined in the need for standardized guidelines and further exploration of the implementation strategies.
Khan, Murad, et al. [12] proposed the integration of artificial intelligence (AI) in cancer treatment, increasing the accuracy of diagnostics and personalization of therapies to improve patient outcomes. The proposal addressed some challenges in traditional cancer care, such as variability in treatment response and a requirement for efficient resource utilization. Results: The results include improved predictive modelling on disease progression and better identification of high-risk populations suitable for tailored interventions. Data security and privacy concerns, healthcare system incompatibility, and the lack of standard procedures all work against its full potential in a therapeutic context.
Bektolotova, Molly, et al. [13] advanced the idea of incorporating artificial intelligence in health for better diagnostic precision and effectiveness in operations. It is realized through a review of existing applications of AI and their potential to automate routine tasks, thereby allowing healthcare professionals to focus on complex patient care. Results have shown that the introduction of AI can substantially improve the health outcomes of patients and lessen the burdens on health systems. Limitations include the concern of algorithmic bias and issues in data privacy, and the requirement of comprehensive regulatory frameworks to handle ethical challenges—all of which have hampered widespread acceptance and implementation of AI technologies in medical practice.
Roppelt et al. [14] advocated the application of artificial intelligence in cancer treatment, making the diagnosis better and more personalized for the care of patients. It applied techniques such as machine learning algorithms and predictive modelling in crunching huge data sets to unlock patterns that traditional approaches may miss. Results were improved and earlier cancer detection, with more effective treatment strategies—each tailor-made to a patient's unique profile. The biggest concern, however, is how to have data privacy and security, challenges in achieving interoperability among the different healthcare systems, and standardized protocols that will make it easy to integrate AI seamlessly into clinical practice.
Chaddad, et al. [15] This paper proposed Federated Learning in healthcare to tackle data privacy and heterogeneity. FL allows decentralized training that aggregates locally trained models placed on a central server without sharing raw data, hence protecting patients' sensitive information. Applied are various techniques to enhance privacy: differential privacy, homomorphic encryption, and secure aggregation. The tasks are classification, segmentation, and analysis of medical data by methods of FedAvg, vertical and horizontal FL, and transfer learning. Results showed that FL can perform comparable to centralized learning in medical imaging and diagnostics. Limitations included dependence on small client numbers, nonidentical data distributions, and high computational costs.
Schünke, Luana Carine, et al. [16] proposed a taxonomy and systematic review of machine learning applications in telemedicine to handle COVID-19 and future pandemics. Motivated by the pressing needs of the pandemic, this study followed the PRISMA guidelines for a rapid literature review, analyzing 16 selected studies. Results showed the effectiveness of telemedicine in triaging, monitoring, and diagnosing patients by using ML-based solutions to provide real-time care while ensuring physical distancing. It also included significant applications in mobile health apps and chatbots. Limitations included reliance on restricted datasets, exclusion of non-English and grey literature, and a lack of studies in non-COVID pandemics—elements that suggest future research to generalize the findings in broader contexts.
Avasthi, Sandhya, et al. [17] proposed leveraging artificial intelligence and machine learning for better mental health care, as the latter may be used for prediction, classification, and treatment based on electronic health records, brain imaging, and mobile monitoring. Inspired by the potential for better diagnosis and improved care of patients facing growing mental health challenges. Results: The use of AI in detecting mental disorders and supporting telemedicine showed promise to bring efficiency and accessibility. Limitations included data quality, ethical concerns, biases, and challenges in real-world implementation, such as overfitting, cybersecurity, and sustaining patient engagement.
Muehlensiepen, Felix, et al. [18] proposed a machine learning approach for predicting telemedicine adoption among rheumatic patients, driven by identifying important factors that could influence TM adoption to improve health delivery. Twelve ML models were compared, and XGBoost showed yielding the most precise findings and AUROC, with 83% and 0.90, respectively. Key predictors were the availability of TM services by rheumatologists, prior TM knowledge, access to the Internet, age, and self-reported health status. Limitations included potential overfitting because of a small sample size, outdated data collection, and biases related to self-selection and non-response.
3. Proposed Methodology
a. Dataset
Continuous and automatic stress monitoring systems are necessary since long-term stress is known to have severe repercussions on well-being. However, no widely used standard datasets in affective computing can a) deliver high-quality data from numerous modality sources and b) incorporate many emotional states for application in wearable stress detection. The dataset introducing WESAD for detecting wearable stress and its effect is available to the public. This multimodal dataset comprises fifteen participants' movements and physiological data collected from a chest- and wrist-worn device during a laboratory investigation. Pulse electrocardiogram, respiration, electromyogram, temperature, electrodermal activity, and threeaxis acceleration are some incorporated sensor modalities. In addition, by including three distinct affective states (neutral, stress, and amusement), the dataset fills a gap in the literature on stress and emotions. Subject self-reports collected from various well-known surveys are also part of the collection [20].
b. AI in Telemedicine
Telemedicine uses telecommunications and digital technology to connect patients and clinicians without in-person visits. Originally developed to improve healthcare access in rural and disadvantaged locations, it is now used worldwide to treat various medical conditions. Due to rapid technological innovation, rising healthcare demand, and the COVID-19 pandemic, it is relevant now. Telemedicine's simplicity, continuity, and global access have made it a landmark in healthcare delivery. Figure 1 shows the integration of telemedicine and AI and its advantages.
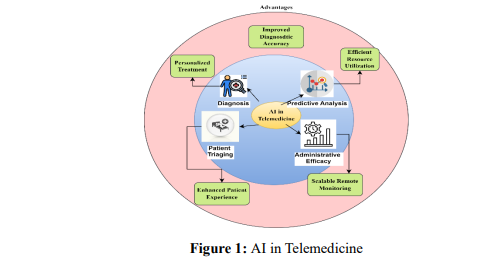
Telemedicine gains machine learning, natural language processing, and computer vision capabilities from AI. AI analyzes medical photos to discover anomalies and enhance diagnosis and results. AI creates individualized treatment plans based on patient data, improving engagement and adherence. AI-driven triage systems and documentation automation improve resource usage. Scalable remote monitoring with AI-powered devices improves chronic disease management and early detection.
c. Objective of the FL-AIVHS method
FL-AIVHS will address telemedicine's biggest issues to improve healthcare delivery. First, federated learning ensures data security by collaborating on AI model training without disclosing raw patient data, ensuring GDPR, HIPAA, and other compliance. This also uses state-of-the-art AI models like Convolutional Neural Networks to improve disease prediction and diagnosis. FL-AIVHS will also provide equitable, high-quality telemedicine services to many various geographical areas, including resource-poor places. Scalable, it can effortlessly adapt to more healthcare providers and greater datasets. FL-AIVHS transforms modern telemedicine with privacy, accuracy, accessibility, and scalability.
d. Overall Workflow of the FL-AIVHS Method
The FL-AIVHS workflow is structured to enable secure, collaborative, and efficient telemedicine delivery. It involves the following step-by-step process. The FL-AIVHS method's workflow is illustrated in Figure 2.
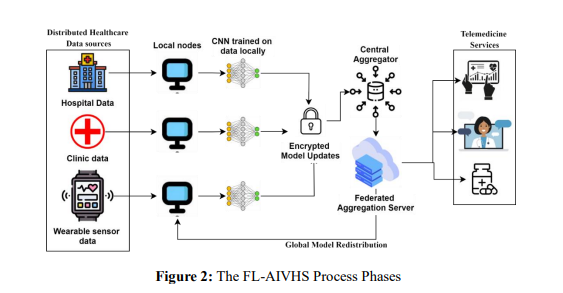
1) Data Acquisition
Source of data: The data for AI-enhanced telemedicine originates from different sources spread across healthcare providers, including hospitals, clinics, and IoT-enabled health monitoring devices. These sources generate a huge variety of data: structured data—for example, electronic health records that provide information on the demography, clinical, and medication history of the patient; unstructured data—for example, doctor's notes, medical imaging, including X-rays and MRIs; and real-time data—for example, vital signs from wearable devices, including heart rate, oxygen saturation, and blood pressure.
Data Anonymization: To protect patients' privacy, any data collected is anonymized and then encrypted before use in AI model training. Data anonymization ensures compliance with privacy standards such as GDPR or HIPAA by removing personally identifiable information.. Let 𝐷 = {𝑑1, 𝑑2, … , 𝑑𝑛} represent the raw dataset, where 𝑑𝑖 contains sensitive information. Anonymization transforms 𝐷 into 𝐷′ = {𝑑1 ′ , 𝑑2 ′ , … , 𝑑𝑛 ′ } such that 𝑑′_𝑖 has no PII but retains clinical utility. Encryption further secures 𝐷′ using an encryption function 𝐸, resulting in 𝐸(𝐷′), which can only be decrypted by authorized systems for training purposes.
2) Data Preprocessing
Preprocessing ensures that the anonymized and encrypted data is compatible and of high quality for training AI models. Scaling numerical features to a specific range, such as [0, 1]. Normalization is done through the equation 1.

where 𝑥 is the raw value, 𝑚𝑖𝑛(𝑥) is the minimum value, and 𝑚𝑎𝑥(𝑥) is the maximum value of the feature. Filtering out irrelevant data or artifacts in signals and images using smoothing techniques like Gaussian filters. Converting unstructured data (e.g., medical images) into standardized formats suitable for AI models, such as tensors for deep learning algorithms.
3) Model Selection and Training Process in FL-AIVHS
The FL-AIVHS is based on cutting-edge AI models for disease detection and medical imaging using Convolutional Neural Networks (CNNs). CNNs have been most suitable for capturing hierarchical features from complex data in X-rays, CT scans, or MRI images. Convolutional, pooling, and fully connected layers make up the fundamental architecture of aconvolutional neural network (CNN) model. Key operations in a convolutional layer could be described as in equation 2.

Where 𝐹𝑖𝑗 refers to the feature map output at position (𝑖,𝑗), 𝑊𝑚𝑛 is the kernel weights, 𝐼(𝑖 + 𝑚)(𝑗 + 𝑛) are the input image pixels, and 𝑏 is the bias term. These features enable the accurate detection and classification of diseases. CNN became a mainstay in tumour identification and retinal image analysis tasks.
Training process in Federated Learning (FL): In Federated Learning (FL), the training process ensures data privacy by making each health provider act as a local node that trains the AI model on its local dataset without transferring sensitive data. First, a global model M with parameters 𝜃 is initialized and sent to all the local nodes. Each node n trains the model 𝑀𝑛 using its local dataset 𝐷𝑛, where the training objective is the minimization of a local loss function, as shown in equation 3.

where ℓ is the loss function (e.g., cross-entropy), 𝑓𝜃 (𝑥𝑖) is the model's output for input 𝑥𝑖 , and 𝑦𝑖 is the ground truth label. After training, the nodes 𝑛 send only the updated parameters 𝜃 (not raw data) to a central aggregator. The central server then aggregates the local updates using techniques like Federated Averaging (FedAvg), as shown in equation 4.

In preparation for the subsequent training cycle, the local nodes receive this aggregated global model. Iteratively updating the parameters and doing local training continues until the global model converges or meets the performance metrics that were set. Compliance with privacy-related legislation is ensured by the AI model, which enhances patient data without compromising its privacy
4) Model Update Sharing in Federated Learning
To secure model updates in transmission, local model parameters, 𝜃𝑛, are first encrypted and then sent to the central aggregator. Encryption is a security layer that prevents unauthorized access or interception of sensitive model updates. Some common techniques for encryption include Homomorphic Encryption and Advanced Encryption Standard (AES). Homomorphic Encryption (𝐸(∙)) (equation 5) enables computations on encrypted data without requiring decryption. This ensures the central server can aggregate encrypted model updates without accessing the raw parameters. The aggregated result is only decrypted after processing. AES Symmetric encryption technique that encrypts data on the local node before transmission is shown in equation 6.

Where 𝐶 is the ciphertext, 𝐸𝑘 is the encryption function using a symmetric key 𝑘, and 𝜃𝑛 are the model parameters.
Communication Protocol: This transmission of encrypted model updates from local nodes to the central aggregator would eventually depend on a very strong secure communication protocol in its integrity, authentication, and protection from possible attacks like man-in-the-middle or replay attacks. It includes Secure Socket Layer/Transport Layer Security, which creates an encrypted channel to securely transfer data after the authentication of both ends through digital certificates. Public Key Infrastructure (PKI) allows for encryption of model updates with the recipient's public key, such that only the holder of the corresponding private key, the central aggregator, can decrypt the data. Integrity is ensured by using Message Authentication Codes (MACs) on the transmitted parameters so that any tampering or unauthorized modifications during transit are detectable. This multi-layer approach ensures the confidentiality and reliability of model update transmission.
5) Disease Prediction and Telemedicine Services
Advanced AI models, integrated into telemedicine services, allow the most accurate prediction of diseases and personalized care for patients. These are driven by predictive analysis and tailored insights derived from patient data to ensure better health outcomes and accessibility.
Predictive analysis: The predictive analysis, by using the most updated global AI model 𝜃𝑔𝑙𝑜𝑏𝑎𝑙, enriched by Federated Learning (FL), makes accurate disease prediction possible for a diverse population of patients. Each local healthcare provider deploys this model and benefits from insights from varied datasets while maintaining data privacy. The first would be data gathering of new patients, including structured inputs like numeric lab results and vital signs and unstructured inputs such as medical images (X-rays and MRIs) and clinical notes. The AI model processes these inputs (𝑥) to predict potential diseases or conditions represented as 𝑦 = 𝑓𝜃𝑔𝑙𝑜𝑏𝑎𝑙(𝑥). where the output (𝑦) can be predicted classes in diseases like diabetes and cancer, or even levels like high, medium, or low risk, or maybe just probability scores. The model improves diagnostic precision, thereby saving health personnel from providing early and effective care.
Personalized Insights: The AI system analyzes the data from patient-specific information, including electronic health records and genomic information, to provide personalized insights that help in formulating optimal treatment recommendations. It makes its recommendations based on predicted outcomes, historical trends, and clinical guidelines for an individualized approach. Starting with the first step in this process, patient profiling combines the predicted disease with contextual factors like age, lifestyle, and comorbidities that build a detailed profile. Advanced algorithms then match the profile with most appropriate treatment options, including medications, lifestyle changes, and rehabilitation programs. The platform carries out virtual results of the different treatments, enabling the professional to establish the best practice most suited to the case. Predictive insights are then shared with the patient, using the benefits of telemedicine with its interactive dashboard for health summaries, live virtual consultations with experts for tailored advice, and AI-driven chatbots assisting with follow-ups and reminders for simple health care.
4. Results and Discussion
a. Performance metrics
This section compares FL-AIVHS with more traditional approaches, such as AI Integration in Cancer Treatment (CT) [12], AI for Diagnostic Accuracy (DA) [13], and FL for Healthcare [15]. The evaluation emphasises key metrics, including model accuracy, reduction of privacy risk, and scalability. Results underline the better performance of FL-AIVHS in achieving higher accuracy, enhanced privacy preservation, and better scalability than these methods. This proves its effectiveness as a strong solution in AI-driven healthcare systems and addresses critical challenges in secure and efficient data utilization.
Model Accuracy: This metric measures how many occurrences were accurately predicted out of all the examples in the set. Equation 7 can be used to calculate it.

𝑇𝑃 (True Positives) and 𝑇𝑁 (True Negatives) are correct predictions and 𝐹𝑃 (False Positives) and 𝐹𝑁 (False Negatives) are incorrect predictions, and accuracy can also be calculated as in equation 8.

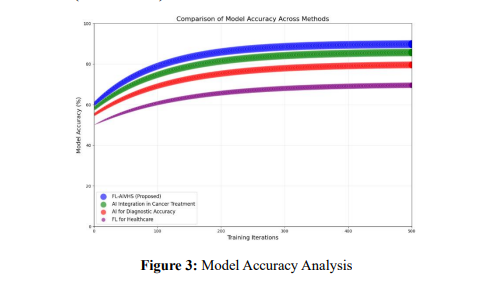
Figure 3 shows a comparison between the model accuracy of FL-AIVHS and some traditional methods like AI Integration in Cancer Treatment—CT [12], AI for Diagnostic Accuracy—DA [13], and FL for Healthcare [15]. The FL-AIVHS reaches the highest accuracy rate of 90%, saturated after 300 iterations with a relatively large bubble size, which means high computational complexity because of Federated Learning and privacy-preserving techniques. AI-CT shows constant improvement up to a peak of 86% in accuracy, with moderate resource demands for personalized cancer diagnostics. The AI-DA reaches an 80% accuracy level with steady growth in this area and balanced resource use, highlighting efficiency. FL-Healthcare reaches 75% using the slowest growth and low computational demands, making it possible even in resource-constrained settings.
Privacy risk reduction: It measures the effectiveness of a technique in reducing the risk of exposing sensitive information. One popular measure is the privacy risk R, which can be quantified as the inverse of the privacy-preserving strength. The privacy risk R decreases as the noise level ϵ or security parameters k increase, for instance, when privacy-preserving methods such as differential privacy or secure multi-party computation are used. The relation can be modeled as in equation 9.

where 𝑅 is the privacy risk (range: 0 to 1, with 0 being no risk and 1 being maximum risk), 𝜖 privacy parameter (higher values correspond to less privacy, range: 0 to 10), 𝜖0 is the threshold privacy parameter where the risk is reduced significantly, and 𝛼 is the steepness of the curve (determines how quickly risk changes). This sigmoid function models a decrease in privacy risk, where larger values of script epsilon initially mean a high privacy risk. As 𝜖 improves, better privacy measures reduce the risk.
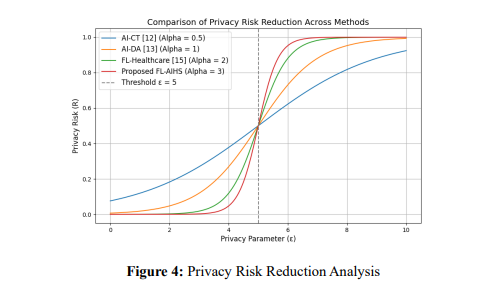
Figure 4 shows the privacy risk reduction analysis by comparing the FL-AIVHS methods and the traditional methods like AI Integration in Cancer Treatment (CT) [12], AI for Diagnostic Accuracy (DA) [13], and FL for Healthcare [15]. The AI in CT follows a slight decrease in privacy risk (α = 0.5) because of less invasive privacy mechanisms; hence, it is usable for moderate privacy requirements. AI for Diagnostic Accuracy offers medium improvement (α = 1) because of trade-offs between computational complexity and privacy. FL for Healthcare achieves steeper reductions (𝛼 = 2) with enhanced mechanisms and focuses on distributed systems. The new FL-AIHS method (𝛼 = 3) shows the greatest reduction, using more sophisticated techniques for full protection at the cost of higher computational demand.
Scalability: Scalability is the ability of a system to scale up to handle increased workloads or resources in an efficient manner. For AI systems, it would generally refer to how their performance improves, or execution time decreases as the number of nodes (e.g., servers, devices) or resources increases. Scalability can be obtained through the equation 10.
b. Performance vs. Resource Demand
A hyperbolic relationship models how system performance (𝑃) improves with increasing resource demand (𝑅) but eventually plateaus. It is shown in equation 11.

Where 𝑃 is the system performance (range: 0 to 1), 𝑅 ia the resource demand (range: 1 to 100), 𝑅_0: Baseline resource capacity, and 𝛽 Efficiency factor (how effectively resources are utilized).
Execution Time vs. Number of Nodes: A distributed system's execution time (𝑇) decreases with an increasing number of nodes (𝑁) but flattens as diminishing returns occur. This can be achieved through equation (11).

where 𝑇 is the execution time (e.g., in seconds). N: Number of nodes (range: 1 to 50), 𝑇0: Initial execution time with a single node. 𝛾, scalability factor (how efficiently nodes improve performance).
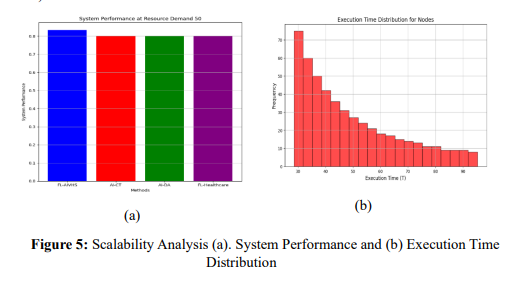
Figure 5 illustrates the plot of execution time versus the number of nodes, bringing out the superior scalability of FL-AIVHS, with the steepest decline in execution time, thanks to its effective mechanism of Federated Averaging (FedAvg) for distributed processing. In comparison, AI-CT and AI-DA show moderate improvement, while FL-Healthcare has the slowest decline due to limited resource optimization. The graph in system performance versus resource demand shows that FL-AIVHS tops the performance and later plateaus, owing to the harnessing of edge computing and efficient AI models like CNNs. Traditional approaches plateau earlier, hence inefficient resource usage, with a lack of mechanisms for distributed training. These are the reasons that significantly limit their scalability and performance. These graphs together show that FL-AIVHS provides better scalability, resource utilization efficiency, and execution efficiency than traditional methods in all aspects due to its state-of-the-art federated learning architecture and privacy-preserving techniques.
5. Conclusion
The FL-AIVHS method is more scalable, private, and better performing than the traditional approaches of AI-CT, AI-DA, and FL-Healthcare. In addition, by using Federated Learning, the execution time of the FL-AIVHS would substantially decrease with an increasing number of nodes and achieve optimum system performance with efficient utilization of resources. Advanced privacy preservation techniques are embedded in maintaining data confidentiality, compliance with regulatory requirements, and reducing the likelihood of breaches. Moreover, the ability of the system to handle decentralized and heterogeneous datasets empowers equitable access to quality healthcare; hence, it is ideal for resource-limited regions. These advantages position FL-AIVHS as a transformative approach to modern telemedicine, addressing challenges in privacy, predictive accuracy, and scalability. Some of the challenges that FL-AIVHS faces include high computational resource requirements, making it less accessible in low-resource settings. Non-identical data distributions across nodes further complicate model convergence and potentially affect predictive accuracy. Such limitations could be overcome by future work in developing lightweight federated learning frameworks to reduce computational costs, efficient communication protocols to reduce overhead, and exploring advanced aggregation techniques to handle non-identical data distributions more effectively in ensuring robust and scalable performance in diverse healthcare environments.
References :
[1]. Rahman, Anichur, et al. "Federated learning-based AI approaches in smart healthcare: concepts, taxonomies, challenges and open issues." Cluster computing 26.4 (2023): 2271-2311.
[2]. Haleem, Abid, et al. "Telemedicine for healthcare: Capabilities, features, barriers, and applications." Sensors international 2 (2021): 100117.
[3]. Nwankwo, Ejike Innocent, et al. "Integrating telemedicine and AI to improve healthcare access in rural settings." International Journal of Life Science Research Archive 7.1 (2024): 59-77.
[4]. Ali-Fakulti, Mohanad Freq, and Jamil Abedalrahim Jamil. "Exploring Pattern Mining with FCM Algorithm for Predicting Female Athlete Behaviour in Sports Analytics."
[5]. Pieczynski, Janusz, Patrycja Kuklo, and Andrzej Grzybowski. "The role of telemedicine, in-home testing and artificial intelligence to alleviate an increasingly burdened healthcare system: Diabetic retinopathy." Ophthalmology and therapy 10.3 (2021): 445-464.
[6]. Nguyen, Dinh C., et al. "Federated learning for smart healthcare: A survey." ACM Computing Surveys (Csur) 55.3 (2022): 1-37.
[7]. Rani, Sita, et al. "Federated learning for secure IoMT-applications in smart healthcare systems: A comprehensive review." Knowledge-based systems 274 (2023): 110658.
[8]. Li, Jiachun, et al. "A federated learning based privacy-preserving smart healthcare system." IEEE Transactions on Industrial Informatics 18.3 (2021).
[9]. Prayitno, et al. "A systematic review of federated learning in the healthcare area: From the perspective of data properties and applications." Applied Sciences 11.23 (2021): 11191.
[10]. Kadir, Muhammad Abdul. "Role of telemedicine in healthcare during COVID-19 pandemic in developing countries." Telehealth and Medicine Today 5.2 (2020).
[11]. Ezeamii, Victor C., et al. "Revolutionizing Healthcare: How telemedicine is improving patient outcomes and expanding access to care." Cureus 16.7 (2024): e63881.
[12]. Khan, Murad, et al. "AI-powered healthcare revolution: an extensive examination of innovative methods in cancer treatment." BULLET: Jurnal Multidisiplin Ilmu 3.1 (2024): 87-98.
[13]. Bekbolatova, Molly, et al. "Transformative potential of AI in Healthcare: definitions, applications, and navigating the ethical Landscape and Public perspectives." Healthcare. Vol. 12. No. 2. MDPI, 2024.
[14]. Roppelt, Julia Stefanie, Dominik K. Kanbach, and Sascha Kraus. "Artificial intelligence in healthcare institutions: A systematic literature review on influencing factors." Technology in society 76 (2024): 102443.
[15]. Chaddad, Ahmad, Yihang Wu, and Christian Desrosiers. "Federated learning for healthcare applications." IEEE Internet of Things Journal (2023).
[16]. Schünke, Luana Carine, et al. "A rapid review of machine learning approaches for telemedicine in the scope of COVID-19." Artificial Intelligence in Medicine 129 (2022): 102312.
[17]. Avasthi, Sandhya, et al. "Augmenting mental healthcare with artificial intelligence, machine learning, and challenges in telemedicine." Handbook of Research on Lifestyle Sustainability and Management Solutions Using AI, Big Data Analytics, and Visualization. IGI global, 2022. 75-90.
[18]. Muehlensiepen, Felix, et al. "Prediction of the acceptance of telemedicine among rheumatic patients: a machine learning-powered secondary analysis of German survey data." Rheumatology International 44.3 (2024): 523-534.
[19]. https://ubi29.informatik.uni-siegen.de/usi/data_wesad.html